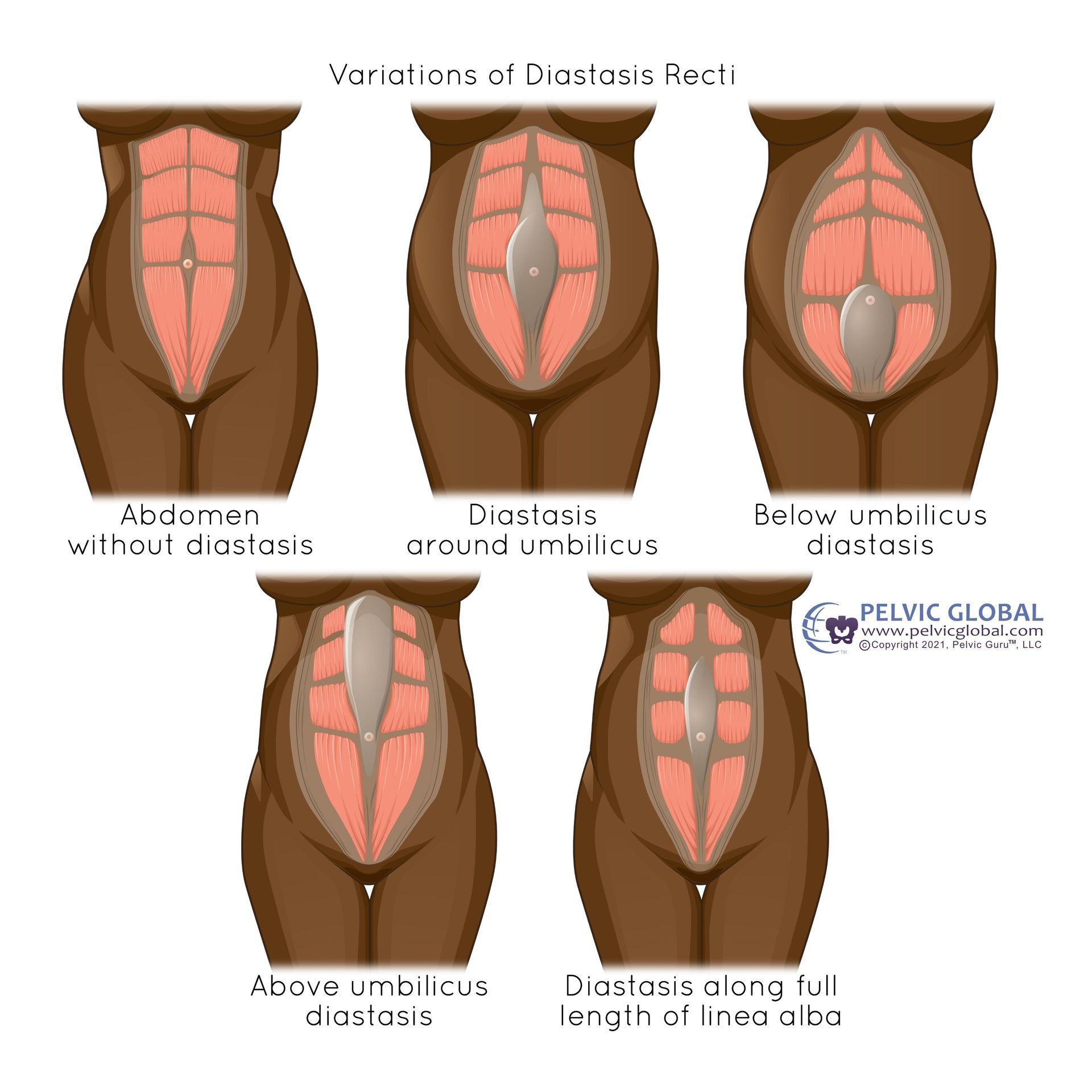
What if exercise alone isn't enough to heal DRA?

Sometimes despite our best efforts, exercise isn't enough to improve diastasis rectus abdominis, aka DRA. Recent studies have been done on other treatment options, alone or with exercise, in an effort to further improve DRA. Let’s run down the list of other things you can try if your DRA isn’t improving enough only with exercise!
TL;DR? Taping your abdominal wall in addition to performing core strengthening exercises can help DRA. Adding electrical stimulation (NMES, or neuromuscular electrical stimulation) to the abdominal wall while doing exercises can also show improvements. And, visceral mobilization (aka massage to the connective tissue that holds up your inner organs) can also help! Not sure what any of that stuff is? Read on below! And know that at Pelvic Love Physio, we are proficient in all of these methods to help you heal your DRA!
Kinesiotape (KT) alone
One small randomized controlled trial (Ptaszkowska 2021) of 24 women did show statistically-significant improvements in DRA width after wearing KT for 48 hours, as compared to a control group that used cloth surgical tape. However, there was no long-term follow-up to see if this effect lasted longer than after the tape was removed.
KT alone or KT plus exercise
Another small randomized controlled trial (Tuttle 2018) split up 30 participants into four groups: exercise alone, KT alone, exercise + KT, and a control group. They were followed for 12 weeks. The taping group wore the tape for 4-7 consecutive days, then took a 2-4 day break, then applied the tape again. The exercise group only did transverse abdominis contractions (abdominal bracing) WITHOUT pelvic floor activation (Kegel) in several positions. These positions included laying on their backs, on their sides, on hands and knees, and in sitting. They did 10 repetitions in each position, 4-5x/week. The KT + exercise group did both of the previously-described procedures, and the control group maintained their normal activity levels. The results? The biggest improvements in DRA were seen in the exercise only group and the exercise + taping group, with no difference between those groups. The taping alone group did show some improvements that were above the minimal clinically important difference (MCID) as described in previous research, but did not reach statistical significance in this study.
Neuromuscular re-education (NMES) alone or NMES plus exercise
NMES is the use of electrical stimulation to help improve the function of weak or underactive muscles. It's not comfortable to say the least! But it can be helpful in certain situations. In this study (Kamel 2017), a group of 60 women was split into two groups: exercise alone, or exercise + NMES (no control group). Each group did the same abdominal strengthening exercises 3x/week for 8 weeks; mostly variations on crunches/curl-ups, but also included some breathing and bracing exercises. Both groups showed statistically-significant improvements across several measures, including width of the DRA. However, the NMES group outperformed the exercise-only group on almost all measures (including width of DRA). If you are interested in trying NMES for your DR, this does need to be done in a PT’s office. And pelvic health PTs are the experts in abdominal wall rehab!
Visceral mobilization
A case series of 3 patients was recently reported in 2021 by Kirk and Elliott-Burke. All patients received at least 4 treatments of various types of visceral mobilization, which is mobilization of the fascia (connective tissue) that surrounds the internal organs. The authors theorize that changes in the uterus size and shape during pregnancy and postpartum recovery places tension on the fascia around it. This tension can increase stiffness in different layers of fascia within the abdomen, thus placing tension on the abdominal wall. By normalizing the tension of the fascial layers inside the abdomen, the abdominal wall then can restore itself to a normal position (e.g. improve/resolve a DRA). In these cases, the primary intervention was visceral mobilization, with minimal exercise interventions specific to each patient. The patients received 6-12 visits in a timespan ranging from 18 weeks to 26 months. All three patients showed complete resolution of their DRAs, plus either resolution of or significant improvement in bladder, bowel, and lower back pain complaints. Additionally, these three women maintained their changes from 6-16 months after discharge.
Takeaways
While none of these methods are fool-proof, all show somewhat promising preliminary results in the treatment of DRA. And all can be performed by us at Pelvic Love Physio! Call or text us today at 309-431-1357 if you have been struggling to heal your DRA, and need a little extra help. We are here for you!
References:
Kirk, B., & Elliott-Burke, T. (2021). The effect of visceral manipulation on Diastasis Recti Abdominis (DRA): A case series. Journal of bodywork and movement therapies, 26, 471–480. https://doi.org/10.1016/j.jbmt.2020.06.007
Kamel, D. M., & Yousif, A. M. (2017). Neuromuscular Electrical Stimulation and Strength Recovery of Postnatal Diastasis Recti Abdominis Muscles. Annals of rehabilitation medicine, 41(3), 465–474. https://doi.org/10.5535/arm.2017.41.3.465
Ptaszkowska, L., Gorecka, J., Paprocka-Borowicz, M., Walewicz, K., Jarzab, S., Majewska-Pulsakowska, M., Gorka-Dynysiewicz, J., Jenczura, A., & Ptaszkowski, K. (2021). Immediate Effects of Kinesio Taping on Rectus Abdominis Diastasis in Postpartum Women-Preliminary Report. Journal of clinical medicine, 10(21), 5043. https://doi.org/10.3390/jcm10215043
Tuttle, L.J., Fasching, J., Keller, A.P., Patel, M., Saville, C., Schlaff, R., Walker, A., Mason, M., & Gombatto, S.P. (2018). Noninvasive Treatment of Postpartum Diastasis Recti Abdominis: A Pilot Study. Journal of Women's Health Physical Therapy, 42, 65–75.